Laceration of Thoracic Duct
content of this page
1- Introduction
2- Anatomical Overview
3- Causes
4- Treatment
Introduction
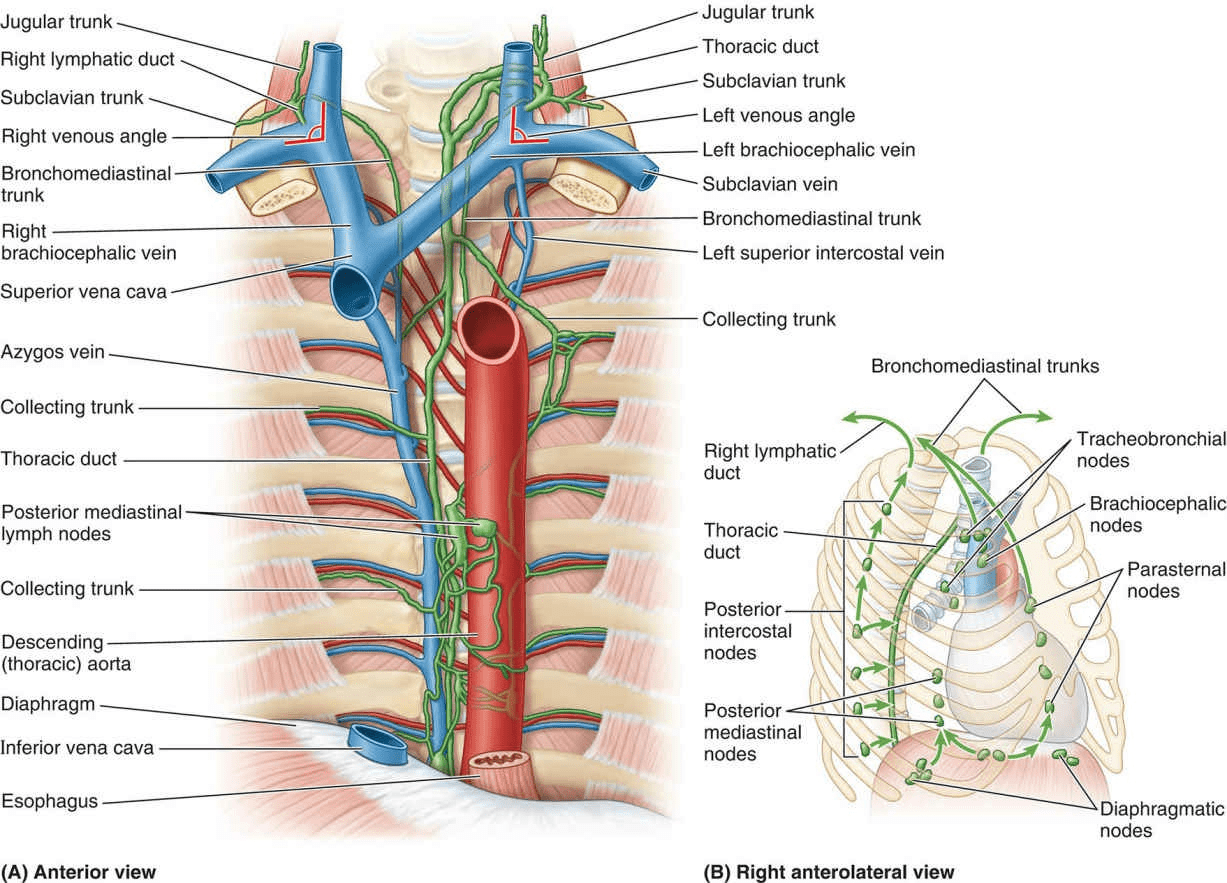
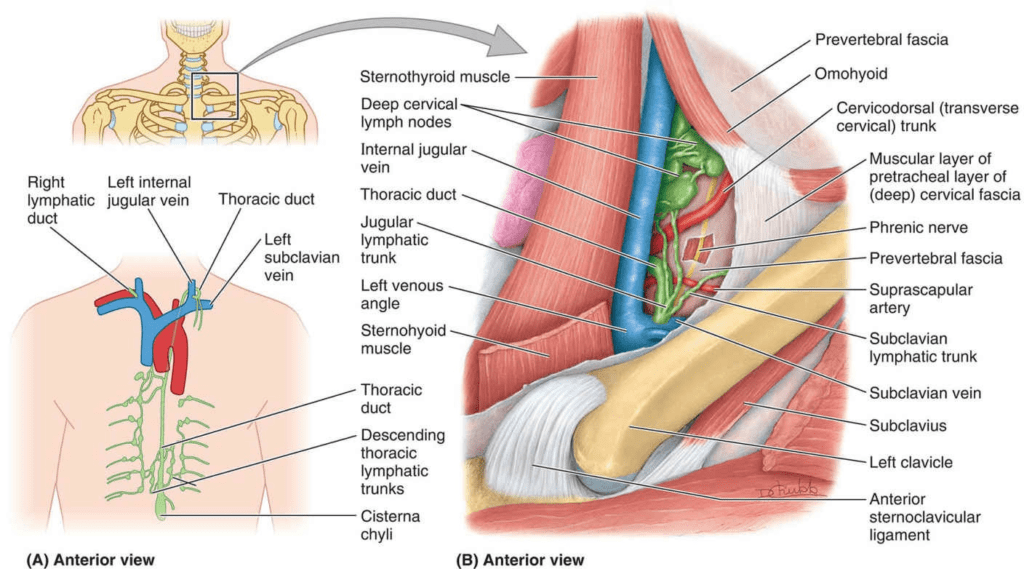
Anatomical Overview
The thoracic duct is thin walled and usually dull white in living persons. However, it may be colorless, making it difficult to identify. Consequently, it is vulnerable to inadvertent injury during investigative and/or surgical procedures in the posterior mediastinum. Laceration of the thoracic duct during an accident or lung surgery results in lymph escaping into the thoracic cavity at rates ranging from 75 to 200 mL per hour. Lymph or chyle from the lacteals of the intestine may also enter the pleural cavity, producing chylothorax. This fluid may be removed by a needle tap or by thoracentesis; in some cases, it may be necessary to ligate (tie off) the thoracic duct. The lymph then returns to the venous system by other lymphatic channels that join the thoracic duct superior
Causes
Trauma: Blunt or penetrating trauma to the chest or abdomen can directly injure the thoracic duct. This trauma may result from motor vehicle accidents, falls, or physical assaults.
Surgical Procedures: Certain surgeries, particularly those involving the thoracic or abdominal regions, can inadvertently damage the thoracic duct. Procedures such as esophagectomy, lung resection, or lymph node dissection carry a risk of injuring the duct.
Medical Procedures: Interventions such as central venous catheterization, thoracentesis (chest tube insertion), or percutaneous procedures in the thoracic or abdominal cavities can accidentally cause damage to the thoracic duct.
Malignancies: Tumors in the thoracic or abdominal regions, such as lymphomas or metastatic cancers, can infiltrate and disrupt the thoracic duct, leading to lacerations.
Inflammatory Conditions: Conditions such as tuberculosis, sarcoidosis, or pancreatitis can cause inflammation and fibrosis around the thoracic duct, increasing the risk of injury during surgical or medical procedures.
Congenital Anomalies: Rare congenital abnormalities, such as abnormal ductal anatomy or cystic dilation of the thoracic duct (known as cystic lymphangioma), can predispose individuals to thoracic duct injury.
Idiopathic Causes: In some cases, the exact cause of thoracic duct laceration may not be identified, and the injury is considered idiopathic.
Treatment
Conservative Management:
- Dietary Modification: Implementing a low-fat diet or medium-chain triglyceride (MCT) diet to reduce the production of lymphatic fluid can help alleviate symptoms and decrease the volume of chyle leakage.
- Nutritional Support: Providing adequate nutrition, including supplementation of fat-soluble vitamins, is essential to prevent malnutrition due to loss of chyle.
Medical Interventions:
- Thoracentesis or Paracentesis: Draining accumulated chyle from the pleural or abdominal cavity through needle aspiration may provide symptomatic relief in cases of chylothorax or chylous ascites.
- Octreotide Therapy: Octreotide, a somatostatin analog, can reduce lymphatic flow and chyle production, potentially decreasing chyle leakage.
Surgical Options:
- Thoracic Duct Ligation: Surgical ligation or clamping of the thoracic duct may be performed to divert lymphatic flow away from the injured segment, allowing the duct to heal.
- Thoracic Duct Repair: In cases of severe injury or persistent leakage, surgical repair of the lacerated thoracic duct may be necessary to restore lymphatic drainage.
Interventional Radiology Procedures:
- Thoracic Duct Embolization: This minimally invasive procedure involves occluding the thoracic duct using embolic agents, coils, or glue, thereby reducing chyle leakage. It is often considered when surgical options are not feasible or have failed.
Medication:
- Antibiotics: Prophylactic or therapeutic antibiotics may be prescribed to prevent or treat infections associated with chyle leakage.
- Pain Management: Analgesic medications may be administered to alleviate discomfort associated with chest or abdominal pain.
Monitoring and Supportive Care:
- Close monitoring of the patient’s clinical status, including serial imaging studies and laboratory tests, is essential to assess the response to treatment and detect any complications promptly.
- Supportive measures such as respiratory support, nutritional supplementation, and physical therapy may be necessary to optimize the patient’s overall condition and facilitate recovery.