
1- Definition
2-Aetiology & Embryology
3- Clinical Features
4- Associated Anomalies
5- Investigations
6- Management Principles
7- Complications
8- Clinical Concepts
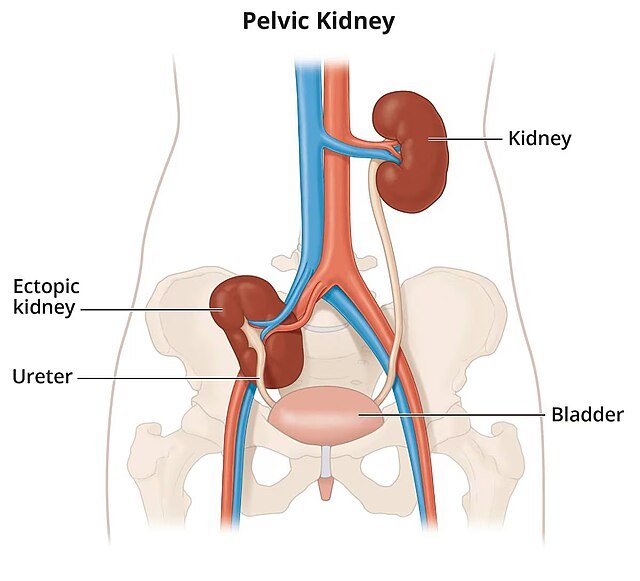
An ectopic kidney is a congenital positional anomaly in which a kidney is located in an abnormal place, usually due to a failure of normal embryological ascent from the pelvis into the abdomen.
Pelvic kidney – located low in the pelvis
Thoracic kidney – herniates above the diaphragm (rare)
Crossed renal ectopia – kidney crosses over to the opposite side, may be fused to the other kidney
In normal development, kidneys form in the pelvis and ascend to the lumbar region by the 9th week of gestation.
Failure of this ascent, or abnormal rotation during migration, results in:
Malposition (e.g. pelvic ectopia)
Malrotation
Abnormal vascular supply
May occur in isolation or as part of a syndromic anomaly (e.g. VACTERL, caudal regression)
Found incidentally during imaging (e.g. antenatal scan or abdominal CT)
Recurrent urinary tract infections (UTIs)
Abdominal or flank pain
Lower abdominal mass (esp. if pelvic)
Hypertension or proteinuria in some cases
Poor renal function if obstructed or dysplastic
Ectopic kidneys may coexist with:
Vesico-ureteric reflux (VUR)
Pelvi-ureteric junction (PUJ) obstruction
Ureteric duplication
Genital tract malformations (especially in females)
Renal dysplasia (underdeveloped nephrons)
Ultrasound: often the first modality
CT/MRI: confirms location, vascular supply, and checks for associated anomalies
DMSA scan: assesses split renal function and detects scarring
MCUG (Micturating cystourethrogram): used when reflux is suspected
MAG3 renogram: evaluates drainage and function over time
No active treatment needed
Educate the patient
Long-term monitoring:
Renal function (eGFR)
Blood pressure
Urinalysis (for proteinuria)
Treat UTIs promptly
If obstruction → Surgical correction
Poorly functioning or non-functioning ectopic kidney with symptoms → may require nephrectomy
Hydronephrosis: due to ureteral kinking or abnormal insertion
Stones: stagnant urine flow predisposes to calculi
Reflux nephropathy: especially if VUR is present
Recurrent UTIs
Hypertension (due to segmental ischemia or scarring)
Impaired renal function if bilateral anomalies
Pelvic kidneys are the most common form of ectopia
Think of ectopic kidney in a child with:
Recurrent UTIs
Single palpable kidney
Absent kidney on ultrasound
Always check for associated abnormalities, especially PUJ obstruction and reflux
Even if asymptomatic, ectopic kidneys need long-term follow-up