Syndrome of inappropriate ADH Secretion (SIADH)
Content of This Page
1- Introduction
2- Causes
3- Symptoms
4- Investigations & Lab Results
5- Prognosis
6- Treatment
Introduction
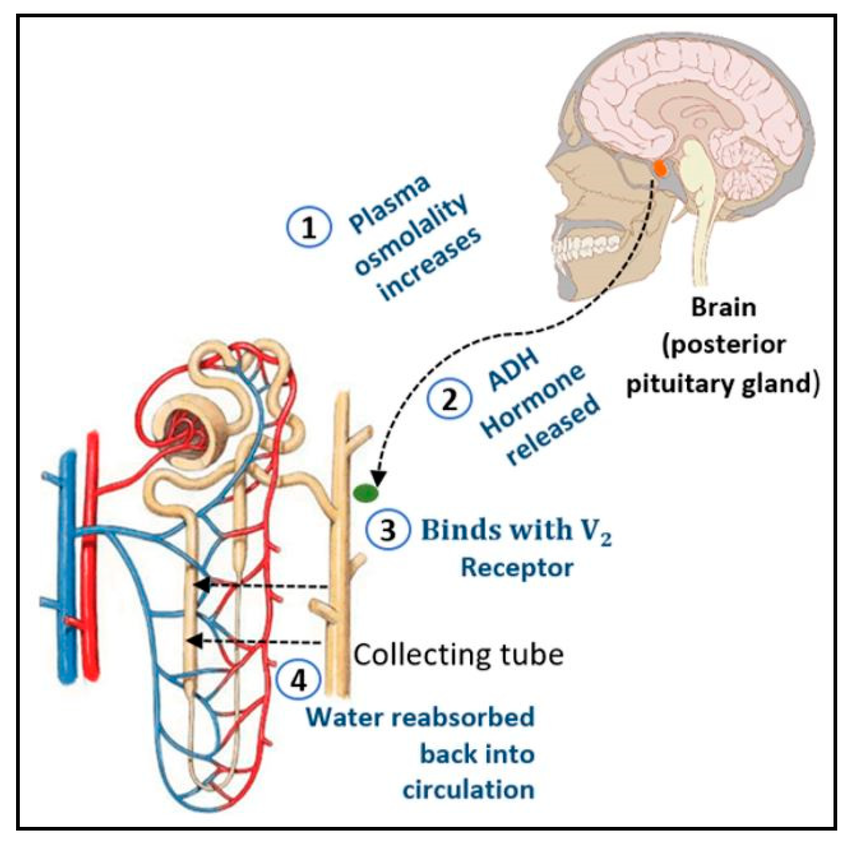
Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH) is a condition characterized by excessive release of antidiuretic hormone (ADH), also known as vasopressin, from the posterior pituitary gland or another source, despite normal or low plasma osmolality. This inappropriate secretion leads to water retention by the kidneys, resulting in dilutional hyponatremia (low blood sodium levels) and decreased serum osmolality.
SIADH can be caused by various underlying conditions such as central nervous system disorders, malignancies (especially small cell lung cancer), pulmonary diseases, certain medications, or idiopathically. Patients with SIADH often present with symptoms related to hyponatremia, ranging from mild nausea and headache to severe neurological manifestations like confusion, seizures, and coma
Causes
Central Nervous System Disorders:
Head trauma
Stroke
Meningitis or encephalitis
Brain tumors
Neurosurgery
Malignancies:
Small cell lung carcinoma (most common tumor-associated cause)
Pancreatic cancer
Prostate cancer
Lymphomas
Pulmonary Diseases:
Pneumonia
Tuberculosis
Acute respiratory distress syndrome (ARDS)
Asthma exacerbations
Medications:
Carbamazepine
SSRIs (Selective Serotonin Reuptake Inhibitors)
Cyclophosphamide
Vincristine
Tricyclic antidepressants
NSAIDs
Other Causes:
Postoperative state (especially after major surgery)
HIV infection
Idiopathic (no identifiable cause)
Symptoms
Mild to moderate hyponatremia:
Nausea
Headache
Fatigue
Muscle cramps or weakness
Confusion or difficulty concentrating
Severe or rapid hyponatremia:
Vomiting
Seizures
Decreased level of consciousness or lethargy
Coma
Respiratory arrest (in extreme cases)
Other signs:
No edema (patients typically appear euvolemic)
Low urine output but urine is concentrated (high urine osmolality)
Investigations & Lab Results
Serum sodium (Na⁺): ↓ (hyponatremia, typically <135 mEq/L)
Serum osmolality: ↓ (usually <275 mOsm/kg, indicating dilution)
Urine sodium: ↑ (usually >20-40 mEq/L, reflecting euvolemic state with normal salt excretion)
Urine osmolality: ↑ (inappropriately concentrated urine, often >100 mOsm/kg despite low serum osmolality)
Blood urea nitrogen (BUN) and serum uric acid: ↓ (due to dilution and increased renal clearance)
Serum creatinine: Normal or ↓
Plasma ADH levels: May be elevated but not always measured routinely
Thyroid and adrenal function tests: Normal (used to exclude hypothyroidism and adrenal insufficiency, which can mimic SIADH)
Prognosis
-Prognosis of SIADH
The prognosis of Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH) largely depends on the underlying cause and how quickly the condition is recognized and treated.
-
If the underlying cause is reversible (such as medication side effects, infections, or surgery-related), the prognosis is generally good with appropriate management.
-
Chronic or malignant causes (like cancer-related SIADH) may carry a more guarded prognosis due to the severity of the primary disease.
-
Untreated or rapidly developing hyponatremia can lead to serious complications, including cerebral edema, seizures, coma, and even death. Prompt correction of sodium imbalance improves outcomes.
-
Careful management is crucial because overly rapid correction of hyponatremia risks causing osmotic demyelination syndrome, a serious neurological condition.
Treatment
1. Treat the Underlying Cause
Stop or change any offending medications.
Treat infections, malignancies, or CNS disorders causing SIADH.
2. Fluid Restriction
Limit fluid intake to usually less than 800–1000 mL/day to reduce water retention.
This is the first-line treatment in most cases.
3. Salt Supplementation
In some cases, oral salt tablets or increased dietary salt help raise serum sodium.
4. Medications
Demeclocycline: Reduces kidney responsiveness to ADH (used in chronic SIADH).
Vaptans (ADH receptor antagonists): Such as tolvaptan, can increase free water excretion but require careful monitoring.
Hypertonic saline (3% NaCl): Reserved for severe or symptomatic hyponatremia (e.g., seizures, coma). Should be given cautiously to avoid rapid sodium correction.
5. Monitoring
Frequent monitoring of serum sodium to avoid overly rapid correction (recommended increase <8-10 mEq/L in 24 hours).
Monitor neurological status closely.