1- Definition & Types
2- Causes (Aetiology)
3- Pathophysiology
4- Clinical Features & Examination
5- Investigations
6- Management
7- Complications
8- Core Concepts
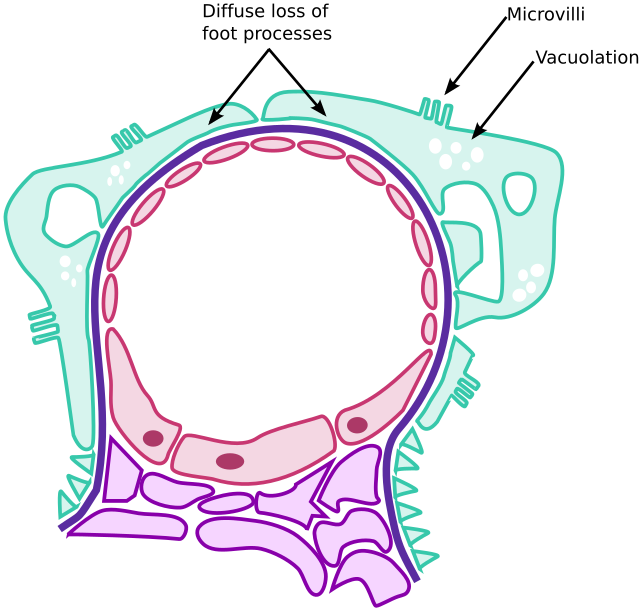
Minimal change disease is a non-proliferative glomerulopathy characterized by:
Normal appearance on light microscopy
Fusion of podocyte foot processes on electron microscopy
It is the leading cause of nephrotic syndrome in children, but also seen in adults.
Type:
Primarily idiopathic
May be secondary to:
NSAIDs
Atopy (allergic conditions)
Haematological malignancies (e.g. Hodgkin lymphoma)
Primary (idiopathic):
Most common, especially in children
Secondary causes:
| Cause | Example |
|---|---|
| Drugs | NSAIDs |
| Malignancies | Hodgkin lymphoma |
| Atopy | Asthma, eczema, allergic rhinitis |
| Infections | Rare, but can trigger relapses |
| Genetic | Suggested in steroid-resistant cases |
The disease involves dysfunction of podocytes → increased permeability to proteins.
No immune complex deposition is seen on immunofluorescence.
Electron microscopy shows effacement of podocyte foot processes.
Believed to be due to a circulating permeability factor, though not yet identified.
-Importantly, there’s no inflammation or proliferation—this distinguishes it from most other glomerulonephritides.
Abrupt onset of nephrotic syndrome:
Generalised oedema
Frothy urine
Hypoalbuminaemia
Hyperlipidaemia
Look for:
Periorbital and pedal oedema
Possible ascites/pleural effusions
Signs of secondary causes (e.g. lymphadenopathy in malignancy)
| Test | Findings |
|---|---|
| Urine dipstick/PCR | Nephrotic-range proteinuria (>350 mg/mmol PCR) |
| Urine microscopy | Bland sediment (no haematuria) |
| Serum albumin | <25–30 g/L |
| Lipids | Elevated (↑ cholesterol, TGs) |
| Renal biopsy | Often not needed in children. In adults or steroid-resistant cases: |
Normal glomeruli on light microscopy
Foot process effacement on EM
Negative immunofluorescence
Fluid and salt restriction
Diuretics for oedema
Statins if persistent dyslipidaemia
Monitor for infection or thromboembolism
High-dose corticosteroids:
Prednisolone 1 mg/kg for 6 weeks
Usually highly effective—> rapid remission
Steroid-dependent or resistant:
Maintenance steroids
Immunosuppressants: cyclophosphamide, calcineurin inhibitors (e.g. ciclosporin, tacrolimus)
Biopsy is warranted if:
No remission after initial steroid course
Atypical features (e.g. haematuria, hypertension)
| Mechanism | Complication |
|---|---|
| Protein loss | Hypoalbuminaemia, oedema |
| Immune globulin loss | ↑ Risk of infection (esp. encapsulated bacteria) |
| Anticoagulant protein loss | Hypercoagulability → DVT, RVT |
| Steroid treatment | Growth suppression, diabetes, osteoporosis |
| Relapses | Common; need for long-term monitoring |
| Feature | MCD |
|---|---|
| Population | Mostly children, some adults |
| Light microscopy | Normal glomeruli |
| EM finding | Podocyte foot process fusion |
| IF finding | Negative (no immune deposits) |
| Response to steroids | Rapid and excellent |
| Risk of CKD | Low (unless steroid-resistant) |
| Associated with | NSAIDs, Hodgkin lymphoma, atopy |